THE STATS ARE UNRELIABLE!
Our COVID Estimate of Situation Web Page:
www.TruthAboutCoronavirus.com
A couple of days ago we posted an OST article questioning the accuracy of COVID-19 statistical reporting. You can see that article HERE. We talked with several experts and came back… confused!
My colleague Robert Goodman, PhD (Biochemistry), pointed out serious inconsistencies in the way COVID cases are being reported which make current statistics, future projections, public announcements and official responses pretty close to absolutely meaningless. Given that so much of our individual and collective well-being hinges on those statistics, announcements and responses, that is a devastating state of affairs. Even allowing for expected government and corporate incompetence, it is hard to see this dismal – and misleading- situation as accidental.
In addition to Dr. Goodman, my co-trustee at Natural Solutions Foundation, Dr Rima (Rima E. Laibow, MD), pointed out, “Garbage In / Garbage Out” referring to the collective unwise “wisdom” about COVID-19, its diagnosis, numbers and significance. She noted unmasks the dirty BIG secret that a March 5, 2020 paper shows that the COVID infection test may give up to 80% false positives.
Potential false-positive rate among the ‘asymptomatic infected individuals’ in close contacts of COVID-19 patients[1]
“Results: When the infection rate of the close contacts and the sensitivity and specificity of reported results were taken as the point estimates, the positive predictive value of the active screening was only 19.67%, in contrast, the false-positive rate of positive results was 80.33%. The multivariate-probabilistic sensitivity analysis results supported the base-case findings, with a 75% probability for the false-positive rate of positive results over 47%. Conclusions: In the close contacts of COVID-19 patients, nearly half or even more of the ‘asymptomatic infected individuals’ reported in the active nucleic acid test screening might be false positives.”
A test which is wrong AT LEAST 80% of the time is worse than worthless. And we know nothing about the rate of false negatives, that is, tests that should come back positive but come back as negative by error.
If a grade of F is earned by something below 65% correct, this test’s grade is H for Horrendous.
And on the basis of these test results, business, schools, lives are being shut down, fascistic powers are removing our rights as citizens, medical and public policy responses are being fashioned and, perhaps worst of all, the carefully orchestrated baying for a mandated vaccine to “save us” is reaching a deafening pitch.
Bill Gates is calling for mandatory vaccination certificates to allow us to travel. Yes, that is the depopulationist Mr. Gates and his charming partner in charity, Melinda.What if we realized that the test itself is meaningless and therefore the horrific daily infection and death statistics are causing ever more fright and panic when a more accurate, and therefore more sober, view of the situation might engender real responses to real problems. If, for example, the deaths reported are any death of any person who might have been exposed to the virus, we have a number that is not much different from the number of deaths that might have occurred naturally during that period. It is primarily the old and the already-ill who are dying. Rather than a true general pandemic, are we measuring the shortening of the time line of hastened, but expected deaths of those already dying?
In fact, we know that 99% of those dying of COVID-19 had other serious illnesses, generally at least 3 of them.[2] Is the real impact of this clearly weaponinzed PLANDEMIC virus to enhance the impact of pneumonia, which the great physician, William Osler, called “the old man’s friend”?[3]
And if that is the primary effect, why are these susceptible people not being given massive doses of IV Vitamin C and Nano Silver 10 PPM as well as Nano Silver 10 PPM by mouth since the clinical experience for both dealing with situations like this is more than abundant, and so is the scientific literature supporting this approach. We are reminded that in 2014, during the Ebola outbreak, WHO, the World health Organization, issued an Ethics Advisory that it was ethical, during an outbreak, to try even “unproven” remedies.
As a side note, jubilation in the ranks of the knowledgeable has broken out because a doctor in New York is giving some of his hospitalized patients IV Vitamin C following nearly 100 years of powerful orthomolecular medicine treating pneumonia and other infectious disorders with IV Vitamin C.
However, the jubilation should, according to Dr. Rima, be very muted indeed since his treatment consists of 1.5 Grams of IV Vitamin C 3-4 times per day for a total upper dose of 6 grams. Dr. Rima uses 16.5 times that much, or 100 Grams as a starting dose for a serious infection and knows what other Advanced Medicine practitioners know: it may be necessary to increase to as much as 200 or even 300 Grams per day in life threatening illnesses like severe COVID-19 pneumonia.
IV Nano Silver, too, is a powerful friend of the patient who wants to live.
So all the jumping up and down over 6 Grams seems as meaningless as the jumping up and down over the meaningless Garbage In, Garbage Out rates of infection, transmission and deaths.
Dr. Rima and I are deeply perplexed by these inconsistencies and serious statistical and clinical deficiencies. Dr. Goodman is also perplexed by the situation and wrote to Dr. Laibow and me the following cogent comments — to which we have added some comments and clarifications interwoven in [bold brackets].
“Since I’d been expressing frustration at trying to follow the current putative array of epidemics laid to Covid-19, I was asked to explain why I’m frustrated. [Other concurrent disease outbreaks of corona and other viruses may well be conflated with COVID.]
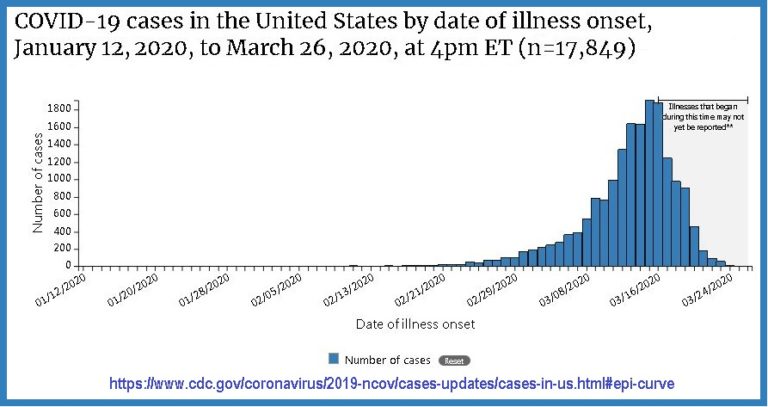
I’d been following incidence data day to day for the USA at https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html#epi-curve , and one frustration was that the CDC in mid-course changed the basis for the data reported in that graph, from using known onset dates for illness to including estimated onset dates. Regardless of which method is more realistic, you can’t follow a trend if the measuring stick is changed.
International data reported at https://www.google.org/crisisresponse/covid19-map are problematic too because there’s no consensus on what to count as “cases”, confirmed or otherwise. Most people seem to assume “confirmation” comes in the form of positive PCR tests for a Covid-19 nucleic acid marker sequence, and that what it is “confirming” is a diagnosis based on signs, symptoms, and/or history of exposure to others testing positive.
However, other “cases” may simply be “confirming” nothing, as when a specimen is tested in the absence of such reason to test. And since we don’t have yet an independent way to confirm positives, we don’t have a reliable way to determine a rate of false positives. We can use as a negative control some random RNA, but that’s not a realistic control, since we don’t know whether the marker sequence is widespread in the population or not.
What is the motivation for testing individuals who have respiratory signs or symptoms? It is estimated that 15% of common cold viruses are coronaviruses, but since most colds don’t progress to the severe lower respiratory signs that have been ascribed to these outbreaks, the significance of a positive Covid-19 RNA sequence in someone with just a history of an otherwise ordinary cold is hard to see, especially when we don’t know at what stage of illness specimens are being taken. [You might test positive to the Wuhan strain of coronavirus but have had symptoms from some other coronavirus. You might test positive as a 4 out of every 5 false positive. You might test positive from having met and NOT gotten sick from COVID-19. You might test negative as a false negative when you really do have the clinical disease or are a carrier.]”
The basis of statistical study on population samples is that the samples be unbiased. There is every reason to think the sampling in these cases is biased, and that the biases differ from place to place and from time to time.[You might be in a country or jail or other environment that only tests people with symptoms, a distinct bias. You might be in a situation in which everyone is tested, whether or not they have symptoms, another distinct bias. The data from these two biased testing situations is not compatible or comparable and, again, the test upon which results and policies are based are so unreliable as to be far worse than random coin tosses, which would be 1 out of 2 positive or negative (heads and tails) where this coin toss is 8 out of 10 making no sense with the other two highly questionable.]
Dr. Robert Goodman
MARCH 29, 2020
Well there we are. The experts are confused because they are looking for logic, not polemic or politics; the statistics are unreliable because they are based on terrible science and horrifyingly bad epidemiology; the actual death-from-COVID-19 rate may or may not be the same as the death rate from other causes coincident to the declared pandemic. If the test that determines if someone is a COVID-19 patient is meaningless, then the declaration that a COVID-19 patient has died or recovered or transmitted the disease is at least equally meaningless.
Despite the fact that we just do not know, the governments of the world, nonetheless, have eagerly and rapidly seized upon this science-absent pretense to shut down whole countries in a highly unsuccessful response (consider Italy for example). And, even more concerning, these same governments have rushed to cancel our civil, civic, legal and personal freedoms as if the constitutions of the allegedly free nations of the world had never been struggled for, won and codified.
In a matter of weeks, we have watched hundreds of years of political freedoms be rushed to the trash bins of expediency, panic and dictatorship.
And the mandatory vaccines to “save us” come next.
Including the vaccine patented 4 years ago according to both NBC News and Newsmax [4]
What is the real agenda behind the massive government-engendered economic crisis, social panic induction and sudden control of nearly every aspect of life “because” of the “widespread” and “extremely deadly” COVID-19 worldwide?
A huge and heavily propagandized boondoggle has emerged: the COVID-19 Bailout. But Cui Bono, as we lawyers like to ask? Who benefits? Well, massive crony corporations and their Governments do. What a surprise! Federal and State agencies will receive the lion’s share of the $2 Trillion COVID Bailout.
Was literally breaking the global economy the best way to stop the viral spread, or would selective self-shielding of the elderly and most vulnerable been a less draconian but effective response?
We, the impacted public need to winnow through the statistics – and the real science behind them – to find reliable data from which we can determine, What is real and what is false in the COVID-19 story? What are the real lessons of COVID-19?
Can individual freedom survive the apparently coordinated “Agenda 2030” global onslaught of COVID-19 repression?
It’s not too early to learn.
Ralph Fucetola JD
Natural Solutions Trustee
Share this message widely! http://www.opensourcetruth.com/covid-19-statistics-are-unintelligible/
————–
[1] https://www.ncbi.nlm.nih.gov/pubmed/32133832?fbclid=IwAR3KtTRFTp9eb0aA-8ThVONEMGeGhecOnjMJtIblbClp8ufahx71HOFSWdg
[2][2] https://www.bloomberg.com/news/articles/2020-03-18/99-of-those-who-died-from-virus-had-other-illness-italy-says
[3] Osler, W, The Principles and Practice of Medicine (1892)
[4] https://www.newsmax.com/newsfront/coronavirus-vaccine-tests-texas/2020/03/05/id/957028/